|
Case Report
A giant colloid cyst of the third ventricle: A case report
1 Neuro-Radiology, Hôpital des Spécialités, Rabat, Morocco
Address correspondence to:
Boujida Nadia
Neuro-Radiology, Hôpital des Spécialités, Rabat,
Morocco
Message to Corresponding Author
Article ID: 100025R02BN2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Nadia B, Ola M, Amal L, Najwa KEC, Meriem F, Mohamed J, Firdaous T. A giant colloid cyst of the third ventricle: A case report. Edorium J Radiol 2024;10(1):1–5.ABSTRACT
Colloid cysts of the third ventricle constitute approximately 1% of all intracranial tumors, and they represent the most prevalent form of neuro-epithelial cysts. They are rare, benign cystic lesions with a wide clinical spectrum, but headache is usually dominant. A large cyst may appear in conjunction with an intracranial hypertension syndrome. Additionally, they can induce obstructive hydrocephalus, resulting in rapid acute neurological decline and, in some cases, sudden death. In this study, our aim is to present the clinical manifestations and radiological features of a giant recurrent colloid cyst of the third ventricle by presenting a case of a 55-year-old female patient, reporting a 2-month history of progressively worsening intracranial hypertension syndrome. The focus is specifically placed on the importance of prompt diagnosis and management to prevent potential life-threatening complications. Minimally invasive modalities, like stereotactic cyst aspiration and neuroendoscopy, are now the preferred techniques of management but present a higher rate of recurrence. Awareness of this condition for early diagnosis and management is fundamental for a better prognosis and patient care.
Keywords: Colloid cyst, Giant colloid cyst, Hydrocephalus, Third ventricle
INTRODUCTION
The term “giant colloid cysts” denotes cysts with a maximal diameter exceeding 3 cm [1], and they are considered rare according to published literature. These cysts present as benign tumors characterized by a gradual growth pattern. They are commonly located at the posterior roof of the third ventricle, posterior to the foramen of Monro. While they generally appear as asymptomatic and small-sized lesions, large colloid cysts typically manifest with headache as a common symptom. Moreover, they often show associations with other symptoms such as altered cognition, nausea, vomiting, gait ataxia, and blurred vision [2]. The potential for high mortality and morbidity arises due to their critical localization and their potential to induce hydrocephalus by impeding cerebrospinal fluid flow [3]. As a result, the prompt identification and management of this lesion are of utmost importance, even considering its benign nature, to prevent potentially life-threatening complications.
CASE REPORT
A 55-year-old female patient arrived at the emergency department, reporting a 2-month history of progressively worsening intracranial hypertension syndrome. This included intermittent headache with an abrupt onset and brief duration. Over time, the headache intensified and became associated with episodes of vomiting.
During the evaluation, the headache was described as constant and severe, affecting both sides. The symptoms were relieved by the supine position, and the neurological examination was negative.
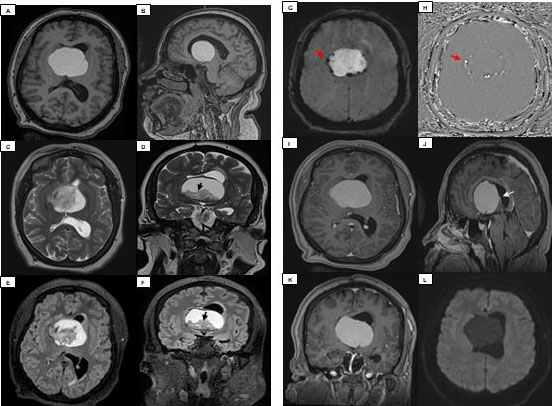
The patient was immediately referred for further radiological assessment. A brain magnetic resonance imaging (MRI) (Figure 1) demonstrated a cyst in the foramina of Monro with typical signal intensities.
Demonstrating a large, well demarcated colloid cyst measuring 5 cm in diameter (52 mL), with a thin capsule, located in the anterior wall of the third ventricle, obstructing the foramina of Monro, and responsible of lateral ventricles dilatation.
The cyst appeared hyperintense on T1, T2, and fluid-attenuated inversion recovery (FLAIR) WI due to its protein content. It also contained a hypointense component on T2 and FLAIR WI, which was attributed to a fluid of thick consistency referred to as “motor oil” (black arrow).
The lesion showed calcifications of its wall as observed on SWI and Pha images (red arrow), with no restriction of diffusion and no enhancement after injection.
Note that the cyst was causing a compression of the hypothalamic region sparing the tuber cinereum, and also exercising a mass effect on both thalamus, and was in intimate contact with the internal cerebral veins (white arrow).
Bilaterally both the body of the caudate nucleus and the internal capsule were repressed.
With the aim of reducing the hydrocephalus, the patient underwent a stereotaxic aspiration as the initial surgical intervention to decrease the volume of the cyst and facilitate the restoration of normal cerebrospinal fluid (CSF) flow.
A follow-up computed tomography (CT) scan (Figure 2) confirmed an insufficient reduction in the cyst volume (28 mL remaining), mainly due to the thick consistency of the cyst, and the CSF obstruction of the foramen of Monro could not be relieved.
The patient’s symptoms were relieved for a short period, but then her intracranial hypertension syndrome recurred.


DISCUSSION
Colloid cysts are congenital, slow-growing, and histopathologically benign tumors. While they have been detected in various parts of the neuraxis [4]. They are commonly situated in the antero-superior part of the third ventricle [5]. They are rarely detected within the pituitary gland and the fourth ventricle [2].
In epidemiological studies, they represent an incidence of 1% per million person-years. They constitute 0.5–1% of all intracranial neoplasms, comprise approximately 15–20% of intraventricular masses [6], and represent 55% of third ventricle’s lesions [5]. The majority of reported cases occur during the third to fifth decades of life with no preference between genders [3].
Colloid cysts arise from the abnormal folding of the primitive neuroepithelium (the paraphysis elements). They contain mucin, old blood (hemosiderin), cholesterol, and various ions, resulting in a wide range of imaging appearance. Histologically, colloid cysts are distinguished by a simple to pseudostratified epithelial lining with interspersed mucous goblet cells and scattered ciliated cells [5].
Although they are histologically benign, they can potentially obstruct the foramen of Monro, leading to acute dilation of the lateral ventricles, which results in hydrocephalus and intracranial hypertension that can be fatal. Compression of the hypothalamus by the cyst, along with the subsequent cardiac reflex can also lead to death [2].
All presentations are primarily associated with elevated intracranial pressure [4], along with irritation of crucial centers located around the third ventricle [7]. The most common presenting symptom is frontal headache which is short and intermittent and can often be relieved by sleep, distinguishing them from space-occupying lesions [8]. This headache is usually associated with nausea and vomiting; however, initial symptoms and clinical syndromes can exhibit significant variability. Additional symptoms comprise, though not exclusively, vertigo, impaired mentation, sudden drop attacks, abrupt leg weakness, blurred vision, and, on rare occasions, seizures. Recent research indicates a prevalence of cognitive symptoms, spanning from anterograde amnesia to gustatory hallucination [2].
Due to their variable content and density, colloid cysts exhibit different imaging characteristics. On CT scans, a significant portion of colloid cysts is often observed as hyperdense in comparison to brain parenchyma. Infrequently, they might present as hypodense or isodense. A thin capsule enhanced with contrast material could be present, and calcification and hemorrhage might be rarely visible as well [8]. Magnetic resonance imaging reveals either intracystic fluid levels or central and peripheral components within the lesion.
Approximately half of colloid cysts appear hyperintense on T1-weighted images, and the remaining cysts exhibit either isointensity or hypointensity [9]. Increased cholesterol content leads to a reduction in T1 relaxation time, resulting in the hyperintense appearance on T1-weighted images [8].
On T2-weighted images, the majority of colloid cysts are of low T2 appearance, related to a thick consistency fluid that can be compared to “motor oil.” Some of the cysts have central low T2 and high peripheral T2 signal, while some are homogeneously high signal [10]. In general, diffusion-weighted images do not typically show any restriction of diffusion in colloid cysts [8].
Radiological differential diagnoses encompass dermoid cyst, ependymoma, craniopharyngioma, or an intraventricular glioma [2].
The treatment is carried out using different modalities including observation and shunting of CSF [4]. Microsurgical approaches like transcallosal, transventricular, and transcortical techniques were traditionally regarded as the gold standard approach.
Newer methods such as neuroendoscopy and stereotactic aspiration of cyst are both minimally invasive procedures [2].
While neuroendoscopy provides a minimally invasive approach through a simple burr hole cyst resection, and is linked to a low complication rate. It offers an excellent short-term outcome. Unfortunately, this approach is associated with a higher rate of cyst recurrence [11]. Prognosis is favorable when timely surgical management is pursued.
CONCLUSION
The origin of colloid cysts remains a subject of debate. However, due to their distinctive location and shape, despite their varied MRI signal characteristics, they usually permit accurate preoperative diagnosis in the majority of patients. The possibility of a colloid cyst in the third ventricle should always be taken into consideration when dealing with cases involving acute headache, nausea, and vomiting. It should be kept in mind that mortality may occur in the patients with hydrocephalus if no surgical intervention is performed. The patients presenting with small-size cysts with no hydrocephalus should be followed up with imaging techniques. This underscores the need for further research to establish the optimal timing for surgical intervention in asymptomatic patients.
REFERENCES
1.
Alkhaibary A, Khairy S. Giant colloid cyst. World Neurosurgery 2022;165: 145-46; Science Direct [cited June 3, 2023].

2.
Bk P, Shrivastava A, Goel G, Panwar H, Kapoor N. A rare, yet classic case of colloid cyst of third ventricle. Cureus 2021;13(7):e16406. [CrossRef]
[Pubmed]
3.
Arslan M, Aycan A, Gulsen I, Akyol ME, Kuyumcu F. Relationship between hydrocephalus etiology and ventriculoperitoneal shunt infection in children and review of literature. J Pak Med Assoc 2018;68(1):38–41.
[Pubmed]
4.
Humphries RL, Stone CK, Bowers RC. Colloid cyst: A case report and literature review of a rare but deadly condition. J Emerg Med 2011;40(1):e5–9. [CrossRef]
[Pubmed]
5.
Hamlat A, Casallo-Quiliano C, Saikali S, Adn M, Brassier G. Huge colloid cyst: Case report and review of unusual forms. Acta Neurochir (Wien) 2004;146(4):397–401. [CrossRef]
[Pubmed]
6.
Diyora B, Nayak N, Kukreja S, Sharma A. Hemorrhagic colloid cyst: Case report and review of the literature. Asian J Neurosurg 2013;8(3):162. [CrossRef]
[Pubmed]
7.
Ravnik J, Bunc G, Grcar A, Zunic M, Velnar T. Colloid cysts of the third ventricle exhibit various clinical presentation: A review of three cases. Bosn J Basic Med Sci 2014;14(3):132–5. [CrossRef]
[Pubmed]
8.
Algin O, Ozmen E, Arslan H. Radiologic manifestations of colloid cysts: A pictorial essay. Can Assoc Radiol J 2013;64(1):56–60. [CrossRef]
[Pubmed]
9.
Kabashi A, Dedushi K, Ymeri L, Ametxhekaj I, Shatri M. Colloid cyst of the third ventricle: Case report and literature review. Acta Inform Med 2020;28(4):283–6. [CrossRef]
[Pubmed]
10.
Gaillard F, Dixon A, Gajera J, et al. Colloid cyst of the third ventricle. Reference article, Radiopaedia.org. [Availalbe at: https://radiopaedia.org/articles/1147]
11.
Vorbau C, Baldauf J, Oertel J, Gaab MR, Schroeder HWS. Long-term results after endoscopic resection of colloid cysts. World Neurosurg 2019;122:e176–85. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Boujida Nadia - Conception of the work, Design of the work, Acquisition of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Messaoud Ola - Acquisition of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Lahfidi Amal - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kettani Ech-Chrif Najwa - Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fikri Meriem - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jiddane Mohamed - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Touarsa Firdaous - Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Boujida Nadia et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.