|
Case Report
Post-traumatic duodenal rupture: A case report
1 MD, Radiology Department, Ibn Sina Teaching Hospital, Mohammed V University, Rabat, Morocco
2 MD, Surgery Department C, Ibn Sina Teaching Hospital, Mohammed V University, Rabat, Morocco
3 MD, Professor, Emergency Radiology Department, Ibn Sina Teaching Hospital, Mohammed V University, Rabat, Morocco
Address correspondence to:
Chaimae Lahlou
MD, Radiology Department, Ibn Sina Teaching Hospital, Mohammed V University, Rabat,
Morocco
Message to Corresponding Author
Article ID: 100026R02CL2024
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Lahlou C, Ihssan HH, Meslouhi K, Hamza O, Malek H, Laila J, Fatima-Zahrae L, Omar EA. Post-traumatic duodenal rupture: A case report. Edorium J Radiol 2024;10(1):6–9.ABSTRACT
Post-traumatic duodenal ruptures are rare. Diagnosis remains difficult due to the anatomical characteristics of the duodenum. Medical observation: the authors report a case of post-traumatic duodenal rupture following a road traffic accident, diagnosed on computed tomography (CT) and treated surgically. Although rare, duodenal ruptures are an emergency for all radiologists. The anatomical complexity of the duodeno-pancreatic region and its proximity to vascular and mesenteric structures explain the rich semiology. Careful radiological analysis is essential to facilitate the surgical procedure. Duodenal rupture is an emergency to be aware of and investigated in all cases of road trauma, especially in the case of blunt trauma. Diagnosis is based on CT scan.
Keywords: CT scan, Duodenum, Rupture, Surgery, Trauma
INTRODUCTION
Duodenal injuries are uncommon, accounting for 0.5–5% of abdominal traumas [1]. This low incidence is attributed to the deep and retroperitoneal location of the duodenum. Anatomical understanding and semiotic analysis through computed tomography (CT) aid in diagnosing post-traumatic duodenal perforations. We report a case of duodenal trauma following a road traffic accident.
CASE REPORT
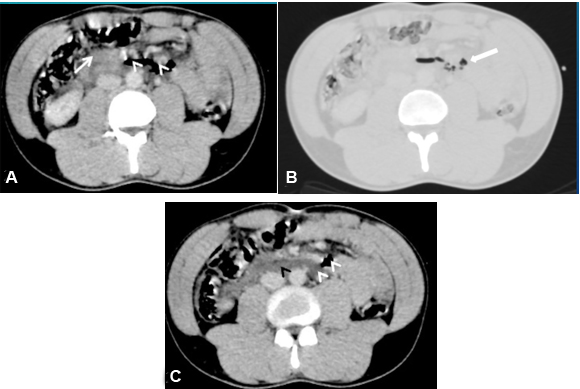
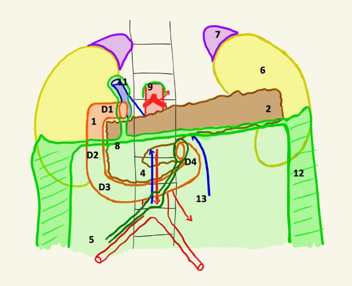
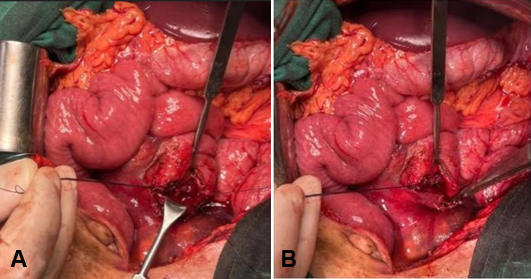
A 32-year-old truck driver was brought to the emergency room after a road accident where he was not wearing a seatbelt, resulting in a frontal impact against the steering wheel. The clinical examination revealed diffuse abdominal tenderness. A CT scan with contrast injection showed retroperitoneal air and fluid accumulation behind the third (D3) and fourth (D4) parts of the duodenum, extending along the central retroperitoneal space (Figure 1), along with a hematoma at the mesentery root (Figure 2). Extra-digestive air bubbles outlined a sizable duodenal wall breach. The pancreas and intra-abdominal organs showed no abnormalities. No vascular or bony lesions, especially in the spine, were detected. The patient underwent exploratory laparoscopy followed by laparotomy, confirming a wall breach affecting 2/3 of the circumference of the D3/D4 angle, with a retroperitoneal collection containing bile and digestive content. Edges were trimmed, and a termino-terminal suture with gastro-entero-anastomosis was performed (Figure 3). The patient had a favorable recovery.
DISCUSSION
Post-traumatic duodenal perforations are rare and associated with an estimated mortality rate of 6–29% [2]. Diagnosis remains challenging, both clinically and radiologically, owing to the anatomical complexity of the duodenum.
The duodenum is the initial part of the small intestine, consisting of four duodenal segments. In terms of frequency, the second segment is the most affected during traumas (36%), followed by the third (18%) and fourth (15%). Multiple injuries are found in 18% of cases [3],[4].
The third segment is horizontal, slightly ascending to the left, crossing in front of the fourth lumbar vertebra. This transverse configuration explains the possibility of compression injuries.
Computed tomography scan is the preferred method for assessing duodenal wall, content, and the peri-duodenal environment.
A duodenal contusion is suspected with focal wall thickening (>4 mm), intramural air bubbles, fat infiltration, and peri-duodenal fluid collection [5]. A duodenal hematoma is characterized by spontaneously dense wall thickening, possibly with upstream gastric distension [5].
Perforation manifests as a parietal discontinuity with adjacent pneumoperitoneum. Retroperitoneal fluid accumulation may be present. In cases of complete rupture, the wall appears dislocated and completely torn, accompanied by pneumoperitoneum, retro-pneumoperitoneum, and retroperitoneal bleeding.
Therefore, semiotic analysis is crucial. In the presence of minor signs like parietal hematoma or peri-duodenal fluid, a conservative approach with a follow-up CT scan at 24 hours is recommended [3]. Conversely, in the presence of major signs, surgical treatment is required. In our patient, a duodenal rupture was identified with a disrupted wall at the D3–D4 junction, along with pneumoperitoneum, retro-pneumoperitoneum, fluid accumulation, and hematoma at the mesentery root.
The surgical treatment of traumatic duodenal perforation involves suturing the breach with an appropriate surgical setup (gastro-entero-anastomosis) or reinforcing the wall with a muscle flap.
CONCLUSION
The duodenum is a deeply located organ that can be affected by both open and closed abdominal traumas. Duodenal rupture is a critical condition that requires prompt recognition. The diagnosis relies on CT scans, and a thorough understanding of anatomy and semiotics is crucial for accurate and precise interpretation.
REFERENCES
1.
Poyrazoglu Y, Duman K, Harlak A. Review of pancreaticoduodenal trauma with a case report. Indian J Surg 2016;78(3):209–13. [CrossRef]
[Pubmed]

2.
Linsenmaier U, Wirth S, Reiser M, Körner M. Diagnosis and classification of pancreatic and duodenal injuries in emergency radiology. Radiographics 2008;28(6):1591–602. [CrossRef]
[Pubmed]
3.
Bradley M, Bonds B, Dreizin D, et al. Indirect signs of blunt duodenal injury on computed tomography: Is non-operative management safe? Injury 2016;47(1):53–8. [CrossRef]
[Pubmed]
4.
Shah S, Khosa F, Rai S, McLaughlin P, Louis L, Nicolaou S. Imaging blunt pancreatic and duodenal trauma. Appl Radiol 2016;45(11):22–8.
5.
Gosangi B, Rocha TC, Duran-Mendicuti A. Imaging spectrum of duodenal emergencies. Radiographics 2020;40(5):1441–57. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Chaimae Lahlou - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hadj Hssain Ihssan - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Kaoutar Meslouhi - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ouzzaouit Hamza - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Hrora Malek - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Jroundi Laila - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Laamrani Fatima-Zahrae - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
El Aoufir Omar - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2024 Chaimae Lahlou et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.